The integration of Artificial Intelligence (AI) into healthcare is revolutionizing the industry in ways that are often invisible to patients. From optimizing hospital operations to the potential for improving clinical decisions, AI’s impact is profound. However, challenges in adoption and data management have historically limited its effectiveness. This blog post delves into the transformative power of generative AI (gen AI), its current applications, the obstacles it faces, and its promising future in healthcare.
Behind the Curve: The Slow Adoption of AI in Healthcare
AI has been used in healthcare for tasks like optimizing workforce allocation and managing inventory, ensuring that facilities are properly staffed and supplied. Despite these applications, the healthcare field lags behind other industries in AI adoption. The sector’s fragmentation, with a vast number of hospitals each operating bespoke systems, complicates the transfer of innovations from one setting to another. Additionally, the siloing of data within hospital walls has blocked the communication of information across institutions.
The Game Changer: Generative AI
Generative AI represents a significant shift in how AI can be leveraged in healthcare. By focusing on refining existing algorithms rather than developing new ones, developers can prioritize data quality, acquisition, and user adoption of gen AI. This shift is generating considerable excitement for its potential to unlock new value in the healthcare domain.
Transforming Data Sharing and Clinical Trials
One notable example of gen AI’s impact is in data handling. Hospitals store vast amounts of data in electronic medical records, including information from devices, scans, and patient histories. The move towards anonymizing or “tokenizing” this data for sharing beyond hospital walls could revolutionize clinical trials by simplifying patient identification processes, therefore enhancing the efficiency and effectiveness of research.
Enhancing Clinical Decision Support
Predictions suggest that gen AI will extend its utility to supporting clinical decisions, a domain previously untouched by this technology. This advancement needs human maintenance due to the technology’s propensity for “hallucinations” or errors, showing the importance of human-AI collaboration.
The Future of Healthcare Consumer Experience
For healthcare consumers, the advancements in gen AI could lead to a more personalized and less friction healthcare experience. From automated documentation during doctor visits to streamlined appointment scheduling, gen AI promises to improve the patient-physician interaction. Moreover, gen AI could offer preliminary guidance for clinical queries, akin to having a doctor in the family, therefore democratizing access to healthcare information.
Optimism for a Healthier Population
The ability of gen AI to facilitate quick, informed decisions and encourage patient compliance with treatments brings optimism for a healthier future. The key to realizing this potential lies in the healthcare industry’s willingness to embrace this technology. Despite current reservations, recognizing gen AI’s capacity to alleviate time-consuming tasks could drive its adoption.
Overcoming Design Challenges
The main hurdle for gen AI is not technological but rather a matter of design. Successful integration into healthcare will depend on creating user-centric systems. As design experts focus on making gen AI more intuitive and accessible, we can anticipate wider acceptance and utilization in the industry.
In summary, even though there are some issues with starting to use gen AI and making it user-friendly, its ability to change healthcare for the better is clear. Gen AI can make healthcare operations more efficient, help doctors make better decisions, and improve the care patients receive. It’s ready to start a new chapter in healthcare with lots of new ideas and improvements. As the healthcare world adjusts to these updates, the main goal will be to use this technology to help create a healthier society with more knowledge.
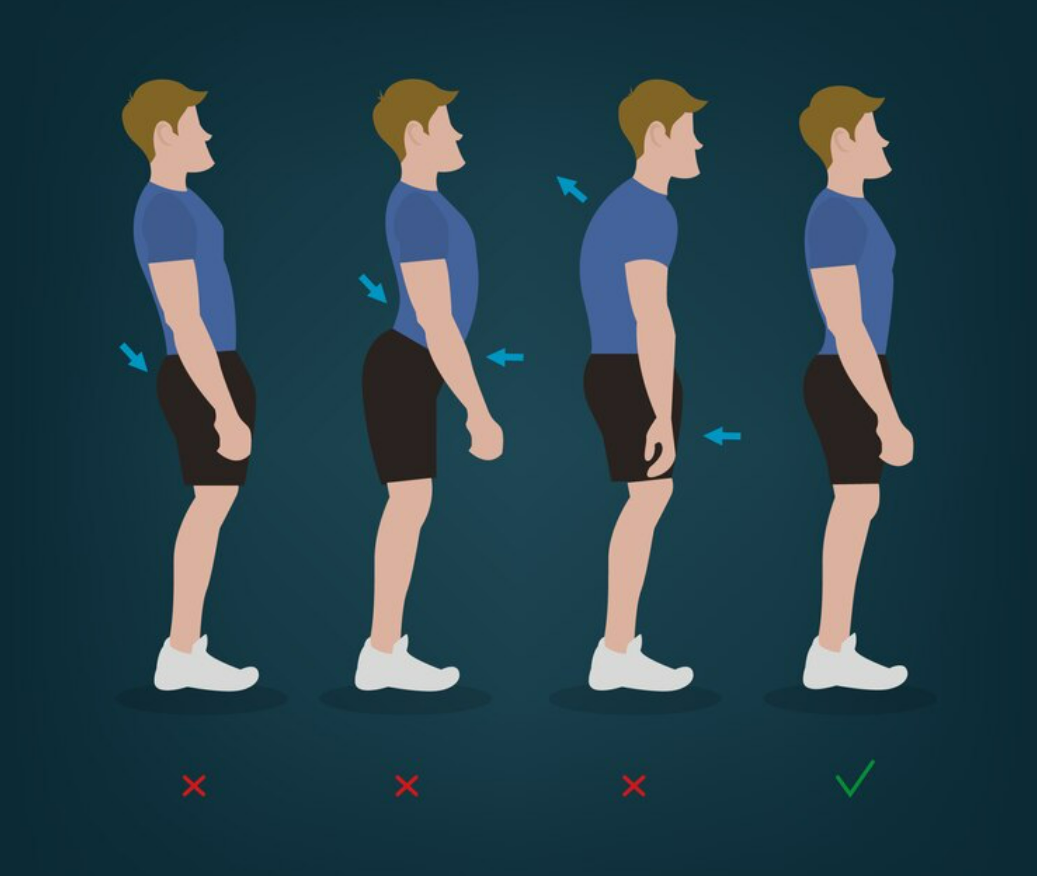
In the ever-evolving landscape of physiotherapy and wellness, posture assessments stand out as a cornerstone for not only preventing but also identifying postural distortion patterns. These patterns, often overlooked, can have far-reaching effects on our overall health and quality of life. Through the lens of evidence-based practice, this post delves into why posture assessments are indispensable in the modern healthcare regimen.
Understanding Postural Distortion Patterns
Postural distortion patterns are misalignments of the body’s posture that can lead to various physical discomforts and musculoskeletal disorders. These patterns are typically the result of prolonged periods of sitting, poor ergonomic practices, or imbalances in muscle strength and flexibility. They can manifest as forward head posture, rounded shoulders, or an exaggerated curvature of the spine, leading to chronic pain, reduced mobility, and impaired functional performance.
The Significance of Posture Assessments
Posture assessments serve as an important diagnostic tool that enables healthcare professionals to identify and analyze these distortion patterns. By conducting a thorough evaluation of an individual’s posture, physiotherapists can pinpoint specific imbalances and areas of tension. This assessment is not just about observing the body’s stance but involves a comprehensive approach, including the analysis of gait, balance, and the functional capacity of various muscle groups.
Prevention and Intervention
The primary goal of posture assessments is not only to identify existing issues but also to prevent future problems. By detecting early signs of postural imbalances, physiotherapists can develop personalized intervention plans. These plans often include targeted exercises, stretching routines, and recommendations for ergonomic adjustments, all aimed at correcting imbalances and enhancing musculoskeletal health.
Empowering Individuals Through Education
An integral part of managing and preventing postural distortion patterns lies in education. Through posture assessments, individuals gain insight into the importance of maintaining proper posture in daily activities. This knowledge empowers them to make conscious decisions about their posture, whether they’re at work, engaging in physical activity, or resting at home.
The Path Forward
In sum, posture assessments are a vital component of a holistic approach to health and wellness. They enable the early detection of postural distortion patterns, facilitate targeted interventions, and play a significant role in educating and empowering individuals. As we continue to navigate a world where sedentary lifestyles are increasingly common, the importance of posture assessments cannot be overstated. By prioritizing posture, we take a significant step towards enhancing our overall health and well-being.
In this blog post, we aim to provide a high-level outlook of what’s in store for AI in healthcare, offering a comprehensive perspective on its transformative role. So, let’s take a close look of the upcoming advancements and potential future developments in the field.
Regulation for Adaptive Algorithms: The regulation of adaptive algorithms has always been a challenge due to their ever-changing nature. Currently, only locked algorithms have received approval. However, this year, the U.S. Food and Drug Administration (FDA) has pledged to address this issue by releasing regulatory descriptions or recommendations to guide the field. To further aid this regulatory process, we will soon be launching a database where users can search for AI healthcare patents, providing valuable insights into future healthcare landscapes.
Specialty-based AI Recommendations and Guidelines: The American College of Radiology has taken a significant step by introducing instructions on submitting studies and papers related to AI technology, along with guidance on how radiologists should approach reading AI studies. Implementing such recommendations and guidelines across all medical specialties would greatly enhance professionals’ understanding and utilization of AI technologies in their respective fields.
Regulation for Large Language Models (LLMs): Given the widespread daily use of large language models like ChatGPT and Google’s MedPaLM by millions of people, including doctors and patients, it is inevitable that some form of regulation will be implemented this year. However, regulating LLMs poses unique challenges, such as interpretability, fairness, and unintended consequences. Tokenization, a crucial aspect of LLMs in natural language processing, currently lacks healthcare regulation and demands attention. A diverse and tailored regulatory framework is essential, considering the broad applicability of LLMs across various domains, with healthcare being the most intricate and critical.
The Debate over Banning Large Language Models: Some countries or regions may opt for a ban on large language models as a response to potential concerns. However, such measures may not effectively address the underlying issues. Users with moderate motivation can easily find ways to circumvent regulations, rendering bans ineffective. A better approach involves leveraging the potential of LLMs through appropriate regulations and user education on working with AI responsibly, rather than resorting to extreme measures.
Exploring Undiscovered Medical Areas for AI Solutions: While AI solutions will continue to flourish in established areas like radiology and oncology, we are also eager to witness the emergence of new fields, including mental health. This exciting prospect indicates that AI adoption will extend beyond automation-prone domains, creating innovative models that combine AI chatbots with human therapists to deliver personalized support to paid subscribers. The integration of AI in these novel areas promises transformative outcomes.
AI in the Everyday Lives of Healthcare Professionals: Millions of doctors, nurses, and healthcare workers are set to explore various AI-based tools that boost efficiency, such as voice-to-text applications for reviewing output. The healthcare sector will benefit from a wide array of AI-driven tools designed not only for medicine but also for a broad range of tasks, from website building to content creation. These tools empower professionals, enabling them to focus more on patient care.
AI’s Trojan Horse in Pharma: Drug Discovery: AI is going to break into the pharmaceutical industry through its application in drug discovery. This area offers substantial potential for cost savings and profit generation, making it an attractive target for AI. With the ability to create new molecules virtually and significantly accelerate the drug discovery process, AI can revolutionize early-stage research, potentially saving years and millions of dollars.
Guidance covers acute, subacute, and chronic pain and replaces 2016 guidelines
Hard thresholds for pain medication doses and duration are no longer promoted through the CDC’s new Clinical Practice Guideline for Prescribing Opioids for Pain.
The new guidance — which covers acute, subacute, and chronic pain for primary care and other clinicians — updates and replaces the controversial 2016 CDC opioid guideline for chronic pain. The 2016 guideline was interpreted as imposingstrict opioid dose and duration limits and was misapplied by some organizations, leading the guideline authors to clarify their recommendations in 2019.
The 2022 recommendations are voluntary and give clinicians and patients flexibility to support individual care, said Christopher Jones, PharmD, DrPH, MPH, acting director of CDC’s National Center for Injury Prevention and Control in a CDC press briefing. They should not be used as an inflexible, one-size-fits-all policy or law, or applied as a rigid standard of care, or replace clinical judgement about personalized treatment, he emphasized.
“Patients with pain should receive compassionate, safe, and effective pain care,” Jones stated. “We want clinicians and patients to have the information they need to weigh the benefits of different approaches to pain care, with the goal of helping people reduce their pain and improve their quality of life.”
The guidance, published in Morbidity and Mortality Weekly Report, addresses four key areas: initiating opioids for pain, selecting opioids and dosages, deciding prescription duration and conducting follow-up, and assessing risk and potential harms of opioids. It suggests that clinicians work with patients to incorporate plans to mitigate risks, including offering naloxone.
The 100-page document indicates opioids should not be considered as first-line or routine therapy for subacute or chronic pain, and points out that non-opioid therapies often are better for many types of acute pain.
“For patients receiving opioids for 1 to 3 months (the timeframe for subacute pain), the 2022 guideline recommends that clinicians avoid continuing opioid treatment without carefully reassessing treatment goals, benefits, and risks in order to prevent unintentional initiation of long-term opioid therapy,” wrote Debbie Dowell, MD, MPH, chief clinical research officer for CDC’s Division of Overdose Prevention, and guideline co-authors in a commentary published in the New England Journal of Medicine.
For chronic pain, clinicians should maximize use of non-opioid therapies and consider initiating opioid therapy only if the expected benefits for pain and function are anticipated to outweigh the risks, Dowell and colleagues noted. When opioids are needed for chronic pain, clinicians should start at the lowest effective dose, evaluate benefits and risks before increasing dosage, and avoid raising dosage above levels likely to yield diminishing returns, they added.
“These principles do not imply that nonpharmacologic and non-opioid pharmacologic therapies must all be tried unsuccessfully in every patient before opioid therapy is offered,” Dowell and colleagues wrote. “Rather, expected benefits specific to the clinical context should be weighed against risks before therapy is initiated.”
The new guideline offers tips for tapering opioids when warranted, but is not intended to lead to rapid opioid tapering or discontinuation, Jones noted. The recommendations do not apply to sickle cell disease-related pain, cancer pain, and palliative or end-of-life care.
The 2022 document incorporated feedback from approximately 5,500 public comments since the new version was first proposed in February, including reactions from people who discussed their experiences with pain or opioid addiction and barriers to pain care. An independent federal advisory committee, four peer reviewers, and members of the public reviewed the draft version.
“The science on pain care has advanced over the past 6 years. During this time, CDC has also learned more from people living with pain, their caregivers, and their clinicians,” Dowell said in a statement. “We’ve been able to improve and expand our recommendations by incorporating new data with a better understanding of people’s lived experiences and the challenges they face when managing pain and pain care.”
The clinical practice guideline supports the HHS Overdose Prevention Strategy, the CDC said. The agency also is providing additional information associated with the guideline to clinicians and patients.
Anxiety is a fear or worry about something happening in the future, such perceived to be stressful, dangerous, or unfamiliar situations. It is a natural response to stress.
Occasional anxiety is completely normal, though. We all experience jitters, nerves or fears from time to time before important events, job interviews, or public speaking. However, experiencing, intense, excessive or persistent anxiety can interfere with the quality of your life and health.
Persistent and intense feelings of anxiety can be hard to control and may hinder your daily activities, job, school work, relationships, and social life. Some people even experience panic attacks characterized by sudden feelings of anxiety or fear that may last for several minutes or longer.
If you have been experiencing anxiety for 6 months or longer that is interfering with your life, you may have an anxiety disorder, such as generalized anxiety, social anxiety disorder and/or phobias. However, even if you experience occasional or mild anxiety, it is beneficial to look into the root causes of the issue and reduce anxiety triggers.
Symptoms of Anxiety
The symptoms of anxiety may differ from person to person, depending on the situation or form of anxiety disorder. Common signs of anxiety may include:
– Increased heart rate
– Rapid breathing
– Feeling tense
– Feeling nervous
– Having a sense of danger
– Restlessness
– Trouble concentrating
– Sense of stress, distress, dread, or worry
– Intense general fear or worry
– Intense fear or worry about a specific situation, place, person, or activity
– Feeling out of control
– Trembling
– Sweating
– Feeling tired or weak
– Gastrointestinal (GI) distress
– Difficulty falling asleep
– Feeling a disconnect between your body and mind
– Painful or worrisome thoughts or memories you are unable to control
– Having difficulty controlling fear or worry
– Urge or behaviors to avoid things that may trigger anxiety
– Nightmares
– Panic attacks
– Overthinking
– Procrastination
– Lack of patience
Nutritional Factors That May Trigger Anxiety
We consider triggers of anxiety, factors such as conflicts in relationships, financial troubles, painful memories, social events, public performances and personal trauma, to list a few. However, you may be surprised to know that your nutrition and overall health may also trigger anxiety. In fact, when your nutrition and overall health is compromised, these commonly considered factors can trigger anxiety even more so.
Let´s take a close look at these nutritional factors:
Blood Sugar
Not eating regularly may lead to a blood sugar drop. Eating a diet high in refined sugar and sugary processed foods also lead to sugar crashes and potentially trigger anxiety. When you eat sugar, your body releases insulin to take care of excess sugar in your bloodstream. However, too much sugar makes it difficult for your body to balance your blood sugar levels and create balance. This leads to sugar crashes and ups and downs that may trigger anxiety, irritability, worry, nervousness, and sadness.
The fact that blood sugar may trigger anxiety is not new knowledge. One of the first research on the topic that blood sugar may trigger anxiety was published in 1966. This study looked at people with reactive or functional hypoglycemia characterized by a relative drop in their blood sugar without reaching the hypoglycemic range.
Subjects experienced anxiety, depression, insomnia, trembling, racing heart, dizziness, and forgetfulness. They were also consuming a diet high in refined carbohydrates and caffeinated beverages. Once they were put on a low-sugar, high-protein, and caffeine-free diet, their blood sugar levels evened out and their anxiety symptoms resolved.
Since this discovery, there have been a number of research studies that have shown how blood sugar levels may trigger anxiety. A 2015 cohort study has shown that a high glycemic load may lead to mood imbalances, hence it may trigger anxiety.
According to a 2016 case report, adding more protein, fat, and fiber to a diet may improve anxiety, mood, concentration, energy, and blood sugar issues of a subject with generalized anxiety and hypoglycemia. Once they returned to her former diet of refined carbohydrates, it triggered anxiety and symptoms returned.
GUT-Brain Axis Dysfunction
Your gut and your brain communicate through the gut-brain axis. One way they connect is through the vagus nerve which begins in the brainstem and travels down into the gut and stimulates bowel motility and the production of neurotransmitters like serotonin in the gut.
The other way your gut and brain communicate is through the microbial species that make up your microbiome. When your microbiome and the gut-brain axis are disrupted it may lead to a number of cognitive dysfunctions and mood disorders including anxiety, depression, obsessive-compulsive disorder (OCD), attention-deficit disorder (ADD), sensory processing disorder, autism, Parkinson’s disease, dementia, and Alzheimer’s disease.
The simplest way to understand the connection between your GUT and your brain is thinking about a time when you felt nervous before a presentation, exam, date, or another event. Chances are that you have felt butterflies in your stomach, nausea, stomach pain, or even diarrhea.
A 2017 scientific review agreed that GUT dysbiosis and inflammation may trigger anxiety, depression, and other prevalent mental illnesses and probiotics may help to prevent or help treat anxiety and depression by restoring normal microbial balance. A 2019 review has shown that probiotic supplements, probiotic-rich foods, and a gut-healthy diet may help to balance your gut microbiome and lower symptoms of anxiety.
Neurotransmitters Imbalances
Neurotransmitters are natural chemical messengers that send information throughout your brain affecting brain health and mood. It is important that they remain balanced to keep a stable mood and mental health.
Neurotransmitters, such as gamma-aminobutyric acid (GABA), glutamate, dopamine, serotonin, and norepinephrine are responsible for regulating your emotions and various functions of your body. They have been shown to trigger anxiety and other mood disorders.
Only glutamate and GABA take up 90% of the neurotransmitters in the body. They are responsible for regulating emotional responses to potentially threatening stimuli that may trigger anxiety.
Glutamate is the main excitatory neurotransmitter in your body. It is involved in every neural pathway in your body, including the ones that affect, relieve, or trigger anxiety. N-methyl-D-aspartate receptor (NMDA) is an important glutamate receptor and ion channel protein located in the nerve cells that are relevant for anxiety.
NMDA may benefit learning and memory, hence it may allow you to unlearn anxiety-provoking behaviors and thoughts and may enhance the benefits of cognitive-behavioral therapy (CBT) to reduce reactions to thoughts and situations that trigger anxiety.
GABA is the main inhibitory neurotransmitter that may help with anxiety relief. This is why doctors may prescribe barbiturates or benzodiazepines that may increase GABA and relieve anxiety. However, these medications do not bind to GABA receptors and also may lead to increased tolerance levels, addictions, toxicity, and serious or even fatal side effects. Instead, there are natural solutions that I will discuss later in this article.
Foods that Can Trigger Anxiety
If you have anxiety, it is extremely important to look at your diet. Inflammatory foods may cause general pain, joint pain, stomachaches, headaches, mood swings, insomnia, and of course, anxiety.
Sugar and Processed Foods
Refined sugar is incredibly inflammatory. When you eat too much sugar, your body simply cannot process it quick enough. As a result, it releases pro-inflammatory messengers called cytokines that may lead to physical and mental health issues.
Processed foods are not only high in sugar, but are usually high in other anxiety-triggering substances such as processed vegetable oils, artificial flavorings, gluten, and additives. Consequently, sugar and processed foods may both trigger anxiety.
Gluten and Grains
Gluten is a protein found in a variety of grains. Gluten is particularly problematic for those with Celiac disease or gluten allergies. However, a large number of the population is sensitive to gluten and may experience inflammation, pain, and health issues from it. Gluten may also trigger anxiety. For some, even gluten-free grains are difficult to digest and trigger anxiety.
Gluten can cause ruptures in the intestines’ fibers causing leaky GUT. It can hinder digestion processes and accumulates toxins which will interfere with the microbiome.
Artificial Flavorings
Artificial ingredients are designed to enhance flavor, texture, color or to extend shelf life.
Aspartame and MSG (monosodium glutamate) are two particularly dangerous artificial flavorings that may trigger anxiety. However, you need to be careful with all artificial ingredients and other additives or preservatives, including MSG, artificial coloring, high fructose corn syrup, guar gum, sodium benzoate, trans fats, and any artificial flavoring. They all may lead to inflammation, increase the risk of chronic disease, and trigger anxiety.
Some of them have the cruel purpose of insatiability, so you will eat certain foods and never feel satisfied, always craving more. It will lead to a chain reaction of inflammation, leaky GUT and, of course, anxiety.
Processed Vegetable Oils
Processed vegetable oils, such as corn oil, canola oil, soybean oil, safflower oil, cottonseed oil, and peanut oil are high in omega-6 fatty acids. This means that they are also inflammatory and contribute to pain and health issues. Processed vegetable oils may trigger anxiety as well.
Conventional Meat Products
The kind of meat you eat absolutely matters. Animals raised for conventional meat products are not treated by the highest of standards. They are treated with hormones and antibiotics and fed with grain instead of grass. As a result, conventional meat products are inflammatory and may trigger anxiety.
Too Much Caffeine
Caffeine may trigger anxiety. Coffee and other caffeinated drinks, such as sodas and energy drinks may cause jittery effects and stimulate a flight or fight response similar to anxiety. Sodas and energy drinks are also full of sugar and artificial ingredients that can further trigger anxiety.
How To Reduce Anxiety Naturally
Conventional treatments of anxiety often include pharmaceutical medications. However, these medications usually serve as a “band aid” without addressing the cause or fully solving the problem. You will be happy to learn that it is possible to reduce anxiety naturally through a nutritious diet, a healthy lifestyle, and appropriate supplementation.
Anti-Inflammatory Healing Diet
An anti-inflammatory healing diet is essential for your overall health, including your mental health. Remove any foods that may trigger anxiety, including refined sugars, processed vegetable oils, processed foods, junk foods, artificial ingredients and flavorings, gluten, grains, conventional meat products, caffeine, and toxins.
Instead, turn to nutrient-dense, anti-inflammatory and healing foods, including leafy greens, such as kale, spinach, and Swiss chard, non-starchy vegetables, such as cucumber and celery, herbs and spices, such as turmeric, ginger, rosemary, and cinnamon, low-glycemic index fruits, such as berries and lemon, healthy fats, such as avocados, organic ghee and butter, and coconut oil, clean protein, such as organic grass-fed beef, pasture-raised poultry, wild-caught fish, wild game, and free-range eggs, nuts and seeds for fiber, and fermented foods, such as kimchi, sauerkraut, and kefir.
Reduce Stress and Prioritize Good Sleep
Anxiety is your body’s natural response to stress. High and chronic stress and a lack of quality sleep may trigger anxiety. To reduce anxiety, it is crucial that you reduce stress and prioritize good sleep.
Try prayer, breathing exercises, daily gratitude, journaling, spiritual practices, nature walks, and quality time with loved ones to reduce your stress levels. Practice positive self-talk and learn to reframe your thoughts.
To support your sleep cycle, aim to go to bed and wake up at the same time each day. Develop a nighttime routine that works for you. Turn off electronics close to bedtime. Engage in relaxational activities and perhaps sip on a calming herbal tea before bed. Invest in a comfortable bed, sheets, and pillows.
Improve Gut Health and Bowel Motility
Your gut affects your brain and mood and compromised gut health and gut flora imbalance may trigger anxiety. Improving your gut health and bowel motility is clearly crucial to prevent anxiety. Eating an anti-inflammatory is the first step, however, there are other ways to support your gut health.
It is really important to calm your body and eat your food in a relaxed state. This will help your body produce enough digestive juices to adequately break down, sterilize and absorb the nutrients you are putting inside of it. When you are stressed out, you will not be able to digest food effectively. If you eat on the go often, it is best to do smoothies and things that are light and easy on your digestive system during these more stressful periods.
Move Your Body Properly
Physical exercise has enormous benefits for your mental health. A lack of movement may trigger anxiety and increase mood imbalances. Research has shown that regular exercise can reduce the frequency and intensity of anxiety and panic attacks.
Exercise regularly, 20 to 30 minutes 5 times a week, and move your body every day. Mix up your routine and find different forms of exercise that work for you. Swimming, hiking, running, and biking are great for cardiovascular health and anxiety relief. Weight lifting, resistance training, kettlebell workouts, and CrossFit are fantastic for your strength.
Yoga has been shown to have both physical and mental health benefits and may help to combat anxiety. Pilates and barre workout is low impact exercises that help to build strength while calming your mind as well. Moving your body doesn’t have to mean structured workouts. Move your body daily by stretching, going for a short walk during lunch, dancing for your favorite song, running around with your kids, and playing with your pets. Remember to have fun.
Consider Seeing a Functional Health Practitioner
Sometimes it’s hard to combat anxiety alone. If you have tried everything and nothing seems to be working, consider finding a functional health practitioner to help you identify the root cause that may trigger anxiety.
Finding the root cause that triggers anxiety is key to figuring out the best natural nutritional and lifestyle solutions to eliminate anxiety from your life. Please do not hesitate to contact Vick Physiotherapy International for professional advice and a free first assessment.
Hello everyone! It has been nearly a year since I last wrote a post! Time literally flies!
In the past year, I have basically focused 100% of my time on my PhD program. Now I have 3 more semesters left, which makes me thrilled to think that I am going to accomplish one of the biggest goals in my career, being a Doctor of Philosophy in Neurosciences with a large application in motor behavior and biomechanics.
However, I have been missing the interaction with my readers and patients, as I am not really using social media nor my blog for professional matters. So today, I officially resumed my school activities, got a brand new computer, and I feel recharged after a full month of holidays here in Europe! So let´s write a post!
Today I would like to talk about joint pain (arthralgia) after COVID-19 infection. I have been hearing from patients, friends and colleagues about this late side effect of this terrible viral infection, so I have done some research about the topic in order to bring the most up to date information for you.
The general answer for joint pain after COVID-19 is plain and simple: your immune system is hyperactive. And what that means?
After contracting the corona virus and/or taking the full vaccine scheme, the immune system is fighting a battle that seems endless. Doctors do not know why it is taking so long for our bodies to adapt and recover from the infection, so the cascade of events is as if we are still sick. The immune system is hyperactive because it understands that both the virus and the vaccine are strangers organisms inside the body, and it is literally putting an entire army of white cells into combat.
As a result, inflammation processes arise, and symptoms such as swelling joints, pain, and general discomfort can occur.
I, personally, did not get infected by the corona virus, however, I am fully vaccinated, and after taking my jabs, I absolutely felt drowsy and extremely tired. I did not add more activities into my routine, and still, I would feel exhausted after a regular day at work and school. I did experience some mild pain and discomfort on both knees, and I totally attributed that as a side effect of the vaccine. But the uncomfortable sensation vanished after 2 or 3 weeks after the jabs, and I carried on with my life and workout routines, although I see that many other people have not overcome those bad symptoms.
Apparently, joint pain will occur all day long, and there is nothing one can do to diminish the sensation. Cold therapy, heat therapy, ultrasound, laser and even deep immersion wouldn´t result positively… What did help a few people I know was to change daily habits in order to help your immune system to take a little break, which means, eating less processed food, avoiding sugar and alcohol, stop using drugs and unnecessary medications, as well as prioritizing a good night of sleep and performing daily workouts for at least 30 minutes.
Those change of habits will not trigger the immune system, and the GUT will do all the work to release the proper neurotransmitters for brain optimization and decrease stress levels. The simple and obvious consequence will be that your blood circulation will improve, so your cells will be nourished. Cortisol levels will decrease, so you won´t be stressed out. Brain fog won´t happen, so you will be able to focus and concentrate more on your daily tasks. The circadian rhythm will regulate, so you will have a proper night of sleep and wake up fresh in the next morning.
So is that the solution for my joint pain after COVID-19? Yes and no. By changing your daily habits, you will simply decelerate the cascade of events that your immune system is working on, so it will be less hyperactive. It is not medical advice nor a protocol to be followed. It is a tip from experience that helped other patients and friends to sooth their pain. And it worked!
Let me know how it works for you by dropping a comment bellow. COVID-19 reactions are still a mystery to the medical field, so collecting evidence is important to build common sense and develop pros and cons for a healthy life.
If you have any enquires or if you want help to change your daily habits, feel free to reach out to me at +1(602)6393726 or send an email to vickphysiotherapy@gmx.com.
Daily thought: “you will always benefit from a healthy body”.
The incidence of ankylosing spondylitis (AS) did not differ between men and women in a large study of military personnel, which called into question the previous assumption of male predominance for this disease.
In a retrospective study that included more than 700,000 military service members, the incidence rate was actually slightly lower for men than for women, at 26.53 versus 31.36 per 100,000, according to Michael H. Weisman, MD, of the Cedars Sinai Medical Center in Los Angeles, and colleagues.
Accordingly, the incidence rate ratio for men was a nonsignificant 1.16 (95% CI 0.91-1.49, P=0.233), the researchers reported online in Arthritis Care & Research. The sole prior population-based study on the incidence of AS in the U.S. was from Olmsted County in Minnesota from 1980 to 2009. In that study’s largely white, homogeneous population, men were three times more likely to have AS than women, but a Canadian report suggested that the incidence amongst women was increasing.
To provide an up-to-date estimate on the incidence of AS — a heterogeneous disease characterized by pain and stiffness of the spine and considerable disability — Weisman’s group analyzed data from the longitudinal Stanford Military Data Repository from 2014 to 2017. Amongst 728,556 active duty personnel, they identified 438 incident cases of AS, for an overall incidence of 27.22 per 100,000 person-years. The greatest difference between sexes was seen amongst individuals ages 24 and younger, amongst whom the incidence rate for women was 21.43 per 100,000 person years compared with 11.11 per 100,000 for men, for an incidence rate ratio of 1.93 (95% CI 1.13-3.29, P=0.015).
A total of 92.69% of patients diagnosed with AS reported having low back pain, and 83.56% had received either x-ray or MRI evaluation of the sacroiliac region. Additional clinical features more frequently experienced by AS patients versus non-AS individuals included (all P<0.001):
Uveitis, 11.42% versus 0.32%
Psoriasis, 7.76% versus 0.70%
Inflammatory bowel disease, 1.83% versus 0.30%
In a multivariate analysis, the adjusted odds of AS were slightly but nonsignificantly lower among men than among women (OR 0.79, 95% CI 0.61-1.02, P=0.072).
However, the adjusted odds ratios rose significantly with increasing age:
Ages 25 to 34, OR 2.62 (95% CI 1.95-3.52)
Ages 35 to 44, OR 5.13 (95% CI 3.79-6.93)
Ages 45 and above, OR 7.30 (95% CI 5.17-10.32)
A further finding was that white patients were significantly more likely to have AS compared with Black patients (OR 1.39, 95% CI 1.01-1.66).
A secondary analysis that required two separate diagnostic codes for AS supported the findings of the primary analysis for the lack of association of AS with male sex, with an adjusted odds ratio of 0.99 (95% CI 0.70-1.40).
In discussing their findings, the researchers pointed out that there were several possible explanations for why their findings differed from those of the earlier Olmsted study. One was that the previous study relied on the modified NY classification criteria for AS, which required the presence of sacroiliac x-ray changes, whereas in this study, almost two-thirds of patients underwent advanced imaging, such as MRI, that could detect more subtle changes.
The use of a military population also might have contributed to the differences in study findings. The majority of the U.S. military is younger than age 30, which is the time frame when AS symptoms first appear. Military personnel have full access to free specialty healthcare, and spinal complaints are addressed by a specific Department of Defense clinical practice guideline.
“Our findings challenge the widely held belief that AS in the U.S. occurs substantially more frequently in males than in females,” the authors concluded.
A limitation of the study was its use of a military cohort, who may be more physically fit and healthier than the broader population. The researchers therefore called for further investigations involving other populations.
Guillain-Barré Syndrome (GBS) is an acquired demyelinating polyneuropathy that often begins in the lower extremities and ascends over time with loss of reflexes, causing muscle weakness, or in the most severe cases, paralysis. Some cases may start a few days or weeks after respiratory or gastrointestinal viral infection. GBS is often reversible.
Researchers from the Maccabi Healthcare Services, the second largest HMO in Israel, searched cases that had been diagnosed by a hospital neurology department, linking them with COVID vaccine records, medical care encounters, and hospital visits after patients received at least one vaccine dose. They conducted a manual review of the electronic medical record of all cases to ensure patients with a GBS diagnosis were accurately identified.
They identified 702 GBS cases between 2000 and 2020; 48% were women and the average age was 53. Of these patients, 579 received one Pfizer vaccine dose and 539 received two doses. The researchers followed these patients for a median of 108 days after the first dose and 90 days after the second. This study is the first to assess the safety of mRNA COVID-19 vaccines in previously diagnosed cases of GBS.
A total of five formerly diagnosed GBS patients were referred to the hospital for neurological concerns after they had the vaccine. Two patients had paresthesia, one had tremor for several months, and one was evaluated for a seizure. These four people were released from the emergency department within a few hours without medical observation. The fifth patient had progressive leg weakness and paresthesia that started soon after she received the first vaccine dose, which lasted for several weeks. She was admitted to the hospital several days after receiving her second dose.
The clinical picture and electrodiagnostic evidence were suggestive of sensorimotor demyelinating polyneuropathy, and the patient was treated with plasmapheresis in the hospital and, by the day of discharge, had a significant improvement in her lower limb weakness and only minor proximal weakness without any sensory disturbance. The analysis was limited because it relied on medical records and diagnosis, the researchers acknowledged. It included only hospital visits and may have underestimated other symptoms that presented only in the community. Nevertheless, any significant serious neurologic concern would probably have been evaluated in a hospital setting.
There were a small number of GBS cases following the swine flu vaccination campaign in 1976, and this question has unfortunately been a vaccination barrier ever since. In reality, patients often are more at risk of neurologic complications such as GBS from the infection than they are from the vaccination designed to prevent it.
It’s important to know that every stroke is different and therefore every recovery will be different. No one can estimate minor stroke recovery time with absolute certainty. Still, there are some patterns worth noting for mild stroke patients. Hopefully these patterns can help you understand what lies ahead on the road to recovery.
To understand the severity of a stroke, it helps to know what the NIH Stroke Scale is.
The NIH Stroke Scale is an assessment tool used to assess the secondary effects of a stroke. This scale helps your medical team “score” you in a variety of areas that can be affected by a stroke, such as movement, vision, and speech.
A high score indicates a significant stroke while a low score implies a mild or moderate stroke. Specifically, a stroke is considered mild when a person scores less than or equal to 5 on the NIH Stroke Scale (out of a possible 42).
Scoring as low as 5 signifies that not many secondary effects are present. For instance, if mobility was affected, the individual is unlikely to be paralyzed. Perhaps the person can lift their affected arm but it may drift down after 10 seconds or so.
It is possible for a mild stroke patient to have significant impairments in one area, but a score as low as 5 would imply that most other areas are unaffected. For example, if speech was severely affected, then mobility and vision remain mostly unaffected for the mild stroke survivor.
Of course, these statements are all generalities. Because every stroke is different, every prognosis will be unique, even for minor strokes.
How Long Does Mild Stroke Recovery Take?
If you had a mild stroke, your stroke recovery timeline will probably be shorter than others with more severe strokes. Because mild strokes do not typically cause major impairments, recovery is usually fast. Sometimes recovery from a mild stroke can occur within 3-6 months. Other times it can take longer.
There are many variables that affect the time it takes to recover. Instead of focusing on recovery time, it can help to focus on the recovery process instead.
When you focus on the steps you can take to recover, you are empowered to take action. And action is how results are made.
Stroke Recovery Process for Mild Stroke
After a stroke, you will spend some initial time at the hospital. But instead of going to an inpatient rehab facility (where patients participate in 3+ hours of therapy per day), mild stroke patients are often discharged straight home.
Generally speaking, if you are able to accomplish the activities of daily living on your own, you are likely to go straight home after the hospital. Your rehabilitation team should instruct you on how to continue rehabilitation at home before discharge.
Once you arrive home, recovery is in your hands. It’s up to you to pursue rehabilitation through various home therapy programs that address your specific needs, especially if it’s not recommended that you go to outpatient therapy.
A Proactive Approach Is Necessary
There’s a myth that mild stroke survivors don’t need to do much to recover, but that’s not true. It’s best to avoid assuming that recovery will take care of itself.
One study noted that “patients with mild stroke are assumed to achieve full recovery with little or no intervention. However, recent studies suggest that such patients may experience persistent disability and difficulty with complex activities.”
This means that a full recovery from stroke is not guaranteed, even for minor stroke survivors. However, even though it’s not guaranteed doesn’t mean it’s not possible.
The ingredient that makes recovery possible is action. Regardless of the size of your stroke, it’s important to participate in rehabilitation in order to maximize your chances of recovery.
With a rigorous therapy regimen, most mild stroke survivors can achieve a full recovery, or get very close to one.
Taking Charge of Your Recovery Time
Instead of participating in therapy at an inpatient rehab facility, most mild stroke patients are discharged home and must keep up with rehab on their own, and/or with outpatient therapy.
Even if you do go to outpatient therapy, it is imperative to participate in a rigorous at-home therapy program as well. This will help patients get the consistent practice that’s necessary to maximize results.
Some mild stroke patients stop pursuing rehab and feel like they are stuck at the level of impairment that they left off with. This doesn’t have to be true.
The brain is capable of changing throughout our entire lives. Whenever we begin to put in the work, the brain will respond. This is why recovery is possible even decades after a stroke.
Again, the essential ingredient is action. You get better at the skills that you practice regularly, no matter how long it has been since your stroke.
Mild Stroke Recovery
Overall, recovery from a mild stroke takes less time than recovery from a massive stroke. The results you see will be dependent upon how consistent you are with rehabilitation.
Because mild stroke survivors often do not go to inpatient rehab, recovery is in your hands. The good news is that, if you keep up with a rigorous home therapy program, you are likely to see a great recovery.
In-home physiotherapy may be better designed by a Physical Therapist, who can personalize treatment and select proper activities in order to increase quality of life. If you want to have a physiotherapy assessment, please give us a call. We are ready to work with you!
If you have been to a physiotherapy clinic in the last few years, then you have almost certainly witnessed, or felt first hand, the technique of foam rolling. Foam rolling is a popular technique that releases tight muscles and mobilizes the network of connective tissues.
When should I consider foam rolling as a treatment?
Scar tissue, adhesion and tightness develop in many ways, namely from trauma, or via less serious injuries, such as repetitive stress and postural dysfunctions. This tightness needs to be dealt with in order to restore proper function and mechanics to the body.
Muscles need to have sufficient strength, but also sufficient flexibility. Whether you are a rugby player, yoga instructor or office worker, it is important to not only have strength but to also have optimal function through a full range of motion.
The Solution?
Foam rolling offers patients an inexpensive, effective and convenient method to reduce scar tissue, breakdown adhesions and improve tissue tone. A patient will use their body weight between the roller and the soft tissue being treated. The patient will roll along the length of the tissue. When a tender spot is found, focus on rolling on that area. The more time spent rolling on the specific area will serve to decrease the degree of pain and tenderness and improve elasticity in the muscle tissue.
Interested in more information on the services we provide? Contact us today!